Have any questions? Feel free to contact us:










Elaborate and Complete
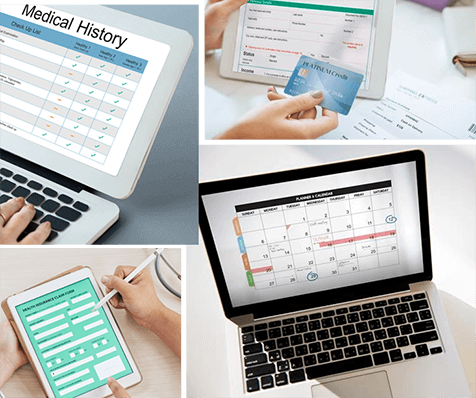
Our services is designed to provide a comprehensive and user-friendly solution for optimizing your billing processes and improving efficiency. Whether you are dealing with insurance claims, patient billing, or other financial matters, our team of experts is here to help you succeed and provide the best possible care to your patients.
Better Interoperability
We help medical practices with their billing and financial management by providing services such as managing payments and tracking patient information. We also offer data analytics to help practices understand and improve their financial performance.

Real-time Intelligence
All your medical billing and medical claim processing and workflows are automated to provide real-time information which is accurate and 100% error-free
